


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://journal.zums.ac.ir/article-1-6419-en.html



✅ This is a report of a 17-year-old wrestler who had suffered from a sport injury during an international competition that led to recurrent shoulder dislocation. Physical examination showed that he had a severe ligamentous laxity.
Humeral avulsion of the glenohumeral ligament (HAGL) lesion is avulsion of the inferior glenohumeral ligament from the anteroinferior humeral neck. It can complicate the anterior shoulder dislocation and it should be considered when evaluating a patient’s magnetic resonance imaging (MRI) results and during arthroscopy. In this report, we present the case of an adolescent professional wrestler who suffered from recurrent anterior shoulder dislocation. He regained his previous sports ability after HAGL and Bankart lesions repair despite having severe ligamentous laxity.
The patient was a 17-year-old wrestler who had suffered from a sport injury in an international competition six months before referring to our clinic. He was right hand- dominant and described the injury to his right shoulder as follows: “When I put my hand over the shoulder of my opponent who had bent over his waist, he raised and turned my arm (abduction and external rotation). I felt an acute and severe pain in my shoulder and could not continue the match”. His shoulder was dislocated and after reduction and four weeks of immobilization, he insisted on resuming his professional wrestling. However, he encountered another dislocation during a noncompetitive exercise.
Physical examination showed pain and apprehension at 90 degrees of abduction. Jerk and sulcus tests had no remarkable results. There was no impingement, muscle atrophy or weakness. The left shoulder examination was normal. Interestingly, the Beighton score for ligamentous laxity was 9, indicating severe ligamentous laxity. Conventional anteroposterior and lateral radiography showed no notable results. However, MRI results demonstrated J sign, indicating a HAGL lesion (Figure 1).

Figure1. J sign , MRI finding of HAGL lesion
We did an arthroscopic repair for the patient. Under general anesthesia examination, the anterior instability was obvious. We entered the joint into the posterior portal, and examined all the 15 areas emphasized by Snyder for diagnostic arthroscopy (1). The anterior-inferior glenohumeral ligament was detached from the humerus in the antero-inferior part and the muscular part of the subscapularis was visualized clearly (Figure 2). The posterior-inferior glenohumeral ligament was intact. There was a small Bankart lesion as detachment of the anteroinferior labrum from the glenoid (Figure 3).

Figure2. From posterior viewing portal,muscular part of SSC is visible clearly as anteroinferior capsule is detached from humerus
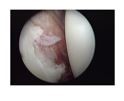
Figure 3. Bankart lesion of antero inferior of Glenoid
First, we made a 5 o'clock portal through the subscapularis tendon without inserting a cannula to prevent iatrogenic damage to the muscle and tendon. Then we made fresh the area of detachment of the ligamentocapsular complex on the humerus (Figure 4). We inserted the anchor suture. Then we repaired the avulsion using a lasso suture passer from the anterior portal.

Figure 4. Using shaver to refresh the insertion site of ligament on the humerus before inserting the anchor suture
After knot tying, we probed the area to be certain about the integrity of the ligamentocapsular attachment (Figure 5). Afterwards, we repaired the Bankart lesion using another anchor suture and finished the surgery.

Figure5. Integrity of ligamentocapsular attachment is probed after the rapair
The post-surgery shoulder immobilization continued for six weeks. Then passive and active shoulder exercises started seriously. In the 3 years follow-up, the patient had no range of motion restriction, had resumed doing sports and had reached his previous ability without any complaint of pain or instability.
Discussion
There are many studies on the pathology of traumatic anterior shoulder instability. The most common pathology seems to be the capsulolabral separation from the glenoid (Bankart lesion) that occurs in about 80% of the cases (2-11). Still, some of the common injuries include capsular laxity or actual humeral insertion avulsion (11-14).
Some of the uncommon shoulder injuries associated with shoulder instability are HAGL lesions. In the presence of a humeral avulsion of the capsule, Nicola seems to be the first to have reported four out of five acute cases of dislocation and six out of 25 recurrent dislocations. This was confirmed with a successive cadaver study in which he dislocated 50 cadaver shoulders (15). Based on his findings the capsule tears off the humerus with hyper abduction (105”) and external rotation; however, there will be a Bankart lesion when hyper abduction is associated with impaction.
In a study by Wolf, 64 shoulders with anterior instability were studied (13). Six shoulders had HAGL lesions, 47 had Bankart lesions, and 11 had capsular laxity. All patients with HAGL lesions had a single traumatic episode as the inciting event in the cause of their anterior instability.
Rhee et al., studied 316 cases undergoing surgery for anterior shoulder instability. They analyzed the cases with HAGL lesions (2%). The range of motion showed 1° loss in forward flexion and 15° loss in external rotation in the last follow-up. They recommended an in-depth examination for Bankart lesion and its associated lesions, including HAGL lesion, to lower the risk of re-dislocation. They stated that the surgeon ought to consider the possibility of a post-surgery loss of external rotation in repairing an HAGL lesion. Thus, s/he should follow an active rehabilitation protocol to have successful results (16).
In a study, Magee investigated a thousand consecutive conventional shoulders. The patients with shoulder pain took MRI to determine the presence of HAGL lesion and its associated lesions (17). A total of 743 patients underwent surgery. 23 HAGL lesions were reported. Among them, 16 HAGL lesions were observed on prospective MR reading and 17 HAGL lesions were observed on retrospective MR consensus reading. Still, he could not observe six HAGL lesions on retrospective consensus reading. There was a 1.6% prevalence amongst all MR examinations, and 2.1% among MR examinations for those who underwent surgery. Hill–Sachs lesion and subscapularis tendon tears were the common injuries associated with HAGL lesions. There were anterior labral tears in only six cases despite Hill–Sachs deformities in 16 patients. Thus, he recommended that we must carefully evaluate the presence of a HAGL lesion in patients with Hill–Sachs lesion without anterior labral tears. Since HAGL lesion was not diagnosed in six of 23 patients, he argued that when the patient is referred late, it is likely that scarring has occurred at the injury site making HAGL lesion diagnosis on MR examination very difficult.
HAGL lesion can complicate the anterior shoulder dislocation in about 2% of cases. MR is useful in HAGL lesions’ diagnosis. MR demonstrates disruption of the inferior glenohumeral ligament at the humeral attachment site on a coronal oblique image. MR arthrogram is useful because it shows extravasation of contrast material. This is through the region of capsular avulsion from the humeral head. An MRI finding associated with HAGL lesions is the “J sign”. It shows that rather than the normal U shape, the inferior glenohumeral ligament is displaced inferiorly with a J shape (18,19). Other shoulder injuries associated with an HAGL injury have a high prevalence. Bui-Mansfield et al., reported 68% incidence for the other associated injuries (18). Magee reported 95% incidence for the other associated injuries (17). Hill-Sachs and subscapularis tendon lesions were the most frequent lesions . In the late referred cases, scaring and thickening of the inferior glenohumeral ligament may interfere with MRI diagnosis. So, an accurate and complete arthroscopic evaluation is necessary especially if Hill-Sachs lesion is not associated with an obvious Bankart lesion in the MRI evaluation of shoulder dislocation.
Concomitant presence of the three different pathologies of shoulder dislocation, including Bankart and HAGL lesions, and severe ligamentous laxity in an adolescent athlete, and full recovery and return to the same level of professional wrestling make this case unique regarding its pathology and arthroscopic treatment result of the anterior shoulder dislocation.
Conclusion
None.
Acknowledgements
None.
Conflicts of Interest
None.
Received: 2021/02/4 | Accepted: 2021/05/10 | Published: 2022/04/1
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright Policy
