


BibTeX | RIS | EndNote | Medlars | ProCite | Reference Manager | RefWorks
Send citation to:
URL: http://journal.zums.ac.ir/article-1-6709-en.html



2- Dept. of Nursing, School of Nursing and Midwifery, Mashhad University of Medical Sciences, Mashhad, Iran
3- Dept. of Nursing, School of Nursing, Sabzevar University of Medical Sciences, Sabzevar, Iran ,
✅EVC should be considered as one of the childhood disorders, which impairs multiple organs as skeletal systems, respiratory disorders and CHD. So, if EVC undiagnosed and remedies poor during childhood, in older ages would reveal disorders.
Ellis-Van Creveld (EVC) syndrome or chondroectodermal dysplasia is a rare genetic disorder. The prevalence of this syndrome ranges from 1:1,000,000 in the general population to 7:1,500,000 in the Amish population (as the most susceptible group) (1, 2). Richard Ellis and Simon Van Creveld discovered EVC syndrome for the first time in 1940 and published a report and essay on this syndrome. The EvC1 and EvC2 genes, located on chromosome 4p16, are responsible for this disorder (3).
The EVC syndrome is characterized by a tetrad of disproportionate dwarfism, bilateral polydactyly, ectodermal dysplasia, and congenital heart disease (CHD) (3). It has a wide range of oral manifestations, the most common of which are natal teeth in the frontal area of the lower jaw and absence of mucosal folds due to the fusion of the upper lip to the margin of the upper jaw. Radiographic findings, such as X-ray, ultrasound, and echocardiography, are the main diagnostic modalities for EVC syndrome. Herein, we describe the case of a newborn with EVC syndrome.
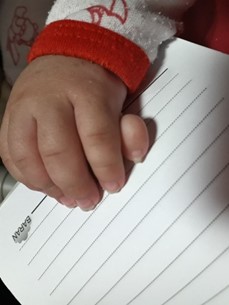
The patient was born through normal vaginal delivery, and there were no complications during labor and delivery. Her weight was 2,950 g at birth, and her height was 54 cm. Her uncle was diagnosed with Down’s syndrome. The symptoms of EVC syndrome were suspected in childhood when she was evaluated for polydactyly (extra digits of the hands) (Figure 1). She had been hospitalized twice since birth due to aspiration pneumonia and atelectasis. In the oral examination, multiple labial frenal attachments were observed in the upper and lower jaws. Her mother noticed shortening of her limbs on ultrasonography in the gestational period. The radiographic findings indicated shortening of long bones. The iliac bones were short and square-shaped, with the acetabulum in a transverse orientation. She showed a slightly elongated chest with short ribs (Figure 2). Based on the cardiac auscultation, her heart sounds were normal, and there was no murmur or echo (normal). Ventricular contraction was also normal, and there were no valve abnormalities or septal defects.
The present study was approved by the Research Ethics of Committee of Sabzevar University of Medical Sciences, Sabzevar, Iran (code: IR.MEDSAB.REC.1400.074).
 |
 |
| Figure 1. Extra digits in hands in a 4- month-old girl with EVC | Figure 2. The iliac bones, acetabula, thorax and ribs in a 4- month-old girl with EVC. |
Discussion
The EVC syndrome or chondroectodermal dysplasia is a rare disease, with an autosomal recessive inheritance pattern (4). This disorder is caused by mutations in two genes, namely, EvC and EvC2, located on chromosome 4 (3). Different organs in the body are affected by EVC syndrome with variable phenotypes (5). The prevalence of this disease at birth is estimated at seven cases per 1,000,000 population. Evidence suggests that it is more common in the older Amish population of Lancaster County (Pennsylvania, USA) (3).
In this case report, we presented the case of a four-month-old girl, whose parents were healthy and non-consanguineously married. Generally, patients with EVC syndrome may present with abnormalities of the thoracic cage, which can cause respiratory disorders (6). Findings suggest a reduction in the functional capacity of the lungs and respiratory failure in infants with skeletal dysplasia, such as EVC syndrome (7). Other unusual findings have been also reported in infants with polydactyly and shortening of the acetabulum in the pelvic cavity. Our patient had a small dorsal vertebral lumbar spine, with short and irregular metaphysics. She had acromesomelic dwarfism, with hexadactyly in the ulnar side of the left hand; there was no hexadactyly in the lower extremities. Some studies suggest that these children have disproportionate limbs, polydactyly, short long bones, and partial chest elongation with short ribs (7-9). Besides, CHD is prevalent in approximately 50-60% of these cases (10). However, our patient had normal preoperative echocardiographic findings.
Some patients with EVC syndrome show hepatic and renal involvement (11); however, our patient had normal hepatic and renal functions. Previous studies used different approaches to treat this disease, and experts from different specialties, including dentists, nutritionists, radiologists, cardiologists, pulmonologists, orthopedists, urologists, pediatricians, ophthalmologists, pediatric neurologists, psychologists, and clinicians, have contributed to research on this disease. Oral problems are among important findings in the diagnosis of this syndrome.
Conclusion
The risk of mortality due to EVC syndrome is high at birth owing to cardiovascular and respiratory complications. Timely treatment protocols can improve the quality of life of these patients and their families and prevent various disorders.
Acknowledgements
We are grateful for the sincere cooperation of the patient's mother, as well as nursing students who assisted us in conducting this study.
Conflicts of Interest
There is no conflict of interest.
Received: 2022/02/10 | Accepted: 2022/10/19 | Published: 2023/03/13
| Rights and permissions | |
 |
This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License. |
Copyright Policy
